
If you are waking up at 3 AM, mind racing, heart pounding, and you cannot explain why, you are not imagining it. You are not anxious. You are not “just stressed.”
Your brain is going through something real, something neurobiological, and it has a name.
As a neurologist and integrative medicine physician, I have sat across from women in their 40s who have been told their sleep problems are “just perimenopause,” handed a pamphlet about sleep hygiene, and sent home. What they were not told is that there is a clear explanation for what is happening in their brain at 3 AM, there are specific labs that can give them answers, and there are evidence-based treatments, including hormone replacement therapy, that can actually help.
When I wrote The Busy Brain Cure, I dedicated significant portions of the book to this exact issue, because I kept seeing the same women in my practice: exhausted, dismissed, and told their labs were normal. This article is the conversation those women deserved to have in the exam room.
Let me give you what you deserve to know.
What Is Actually Happening to Your Sleep in Perimenopause
The 3 AM wake-up is not random. It is not anxiety. It is neurobiology.
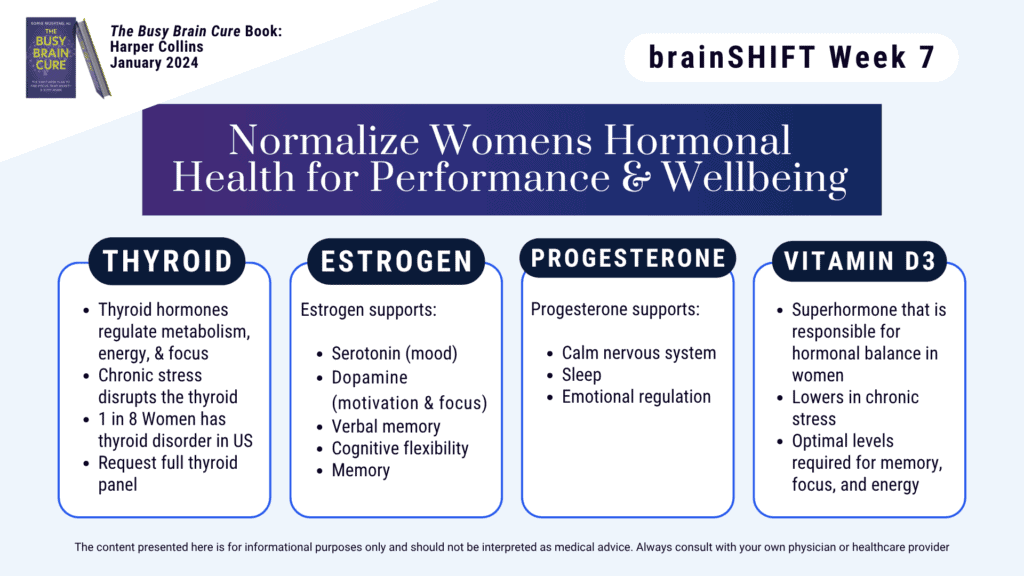
As progesterone declines during perimenopause, your brain loses one of its most powerful natural calming signals. Progesterone directly activates the same receptors that sleep medications target, the GABA-A receptors. Layer on top of that the body’s natural cortisol rise in the early morning hours, and you have a brain that is chemically primed to wake up, race, and refuse to settle, even when you feel no physical symptoms at all.What most women do not know is that thyroid function and morning cortisol levels are also quietly shaping this picture, and those labs are rarely checked at a routine visit. This is why so many women are told their labs are “normal” when, in fact, the full picture has never been evaluated. In The Busy Brain Cure, I walk through exactly why the standard lab panel most doctors order is incomplete, and what the missing pieces actually mean for your sleep, focus, and energy.
Why Temperature and Anxiety Wake-Ups Are the Same Problem
You may have noticed that sometimes you wake up overheated, and sometimes you wake up anxious, and you cannot always tell which came first. That is because they are coming from the same place.
The hypothalamus is command central for both your body’s thermostat and your sleep-wake cycle. During perimenopause, the neurons that become hyperactive from estrogen and progesterone loss sit right next to the area that governs how and when you fall asleep. What feels like waking up anxious and what feels like a temperature spike are often the same hypothalamic event expressing itself in two different ways.This is exactly why I tell women that getting a full hormone panel is not optional information. It is the roadmap to understanding what your brain and body are actually asking for. And it is one of the reasons I built an entire chapter in The Busy Brain Cure around hormone health as a foundational pillar of brain performance, not a side conversation.
Does the Research Support Temperature Regulation Tech, Like a Smart Mattress?
The science here is real, and it is more than marketing.
Pilot studies on cooling mattress technology have shown meaningful reductions in vasomotor symptoms and measurable improvements in sleep quality scores. The most recent data from SLEEP 2025 showed roughly a 10% improvement in sleep quality with optimized temperature programming. That is a real signal.
That said, I frame this honestly with my patients. A cooling mattress can be a genuinely useful adjunct to treatment. It is not a replacement for addressing the underlying hormonal and neurological drivers of what is keeping you awake. If your estradiol and progesterone levels have never been evaluated, a cooling mattress may help you feel more comfortable tonight. It is not treating the root cause.
“We spent two decades scaring women away from hormone therapy based on research that has since been significantly reinterpreted. What we know now is that for many women in perimenopause, HRT is not just about managing symptoms. It is about protecting the brain, protecting sleep architecture, and protecting long-term cognitive health.”
— Dr. Romie Mushtaq
The Most Underrated Things Perimenopausal Women Can Do to Improve Sleep
There are two answers here, and most women are missing both.
The first is getting the right labs. That means a full thyroid panel, a morning cortisol level, and a complete hormone panel that includes estradiol, progesterone, and testosterone. These numbers tell you what is physiologically driving your sleep disruption. Without them, you are guessing. In Chapter 16 of The Busy Brain Cure, I provide a complimentary list of the exact labs to request at your next appointment, including how to talk to your doctor about why each one matters. Print it out and bring it with you.
The second is having an honest conversation about hormone replacement therapy. For women who are candidates, HRT remains one of the most evidence-based and underutilized tools we have for restoring sleep, stabilizing mood, and protecting brain health during the menopausal transition. The fear around HRT kept too many women suffering unnecessarily for too long, and that narrative needs to change. There is also a third tool worth knowing about, one that is almost never mentioned: Cognitive Behavioral Therapy for Insomnia, known as CBT-I. In a rigorous clinical trial called MS-FLASH, CBT-I outperformed estradiol, antidepressants, yoga, and omega-3 supplementation for improving sleep in menopausal women. It retrains the thought patterns and behavioral habits that keep a sleep-deprived brain in a state of hyperarousal, and it delivers results that last. I break down the CBT-I steps in Chapter 11 of The Busy Brain Cure as a practical sleep challenge you can begin on your own, alongside guidance on hormonal therapy, so you are addressing this from more than one direction at once.
When Does Disrupted Sleep in Your 40s Warrant a Doctor Conversation?
If you have been waking consistently, feeling unrefreshed no matter how many hours you sleep, or noticing that your mood, memory, and focus are suffering, that conversation with your doctor should have already happened.
One of the most commonly missed diagnoses in women at midlife is sleep apnea. Women present very differently than men, with fatigue, low mood, brain fog, and unrefreshing sleep rather than obvious snoring, so it gets attributed to perimenopause and goes unscreened. It is one of the most consequential missed diagnoses I see in this population.
Come to your appointment prepared. Bring a two-week sleep log and a list of every symptom, including brain fog, mood changes, and memory slips. Then ask for these specific things: a full thyroid panel, a morning cortisol level, and a hormone panel including estradiol, progesterone, and testosterone. And ask directly: “Is hormone replacement therapy an option for me?”
That question deserves a real answer, not a dismissal.
What to Ask for at Your Next Appointment
Here is what I recommend you bring to your doctor. (You will also find a ready-to-use version of this list in Chapter 16 of The Busy Brain Cure.)
- A two-week sleep log noting wake times, symptoms, and how you feel in the morning
- A list of all symptoms including brain fog, mood changes, and memory difficulties
- A request for a full thyroid panel (not just TSH)
- A request for a morning cortisol level
- A request for a complete hormone panel: estradiol, progesterone, and testosterone
- A direct question about whether hormone replacement therapy is appropriate for you
- A question about whether you should be screened for sleep apnea
You deserve answers, not a handout on sleep hygiene.
If you want to go deeper, The Busy Brain Cure is the place to start. It walks you through the brain science behind sleep disruption, the labs worth requesting, the sleep challenge rooted in CBT-I principles, and what it means to protect your brain through every season of life.
And take the Busy Brain Test to understand what may be driving your sleep disruption, focus challenges, and fatigue right now.If your organization is navigating burnout, change fatigue, or the wellbeing of a workforce in transition, let’s talk about bringing brainSHIFT to your team.
Frequently Asked Questions
Why do I wake up at 3 AM during perimenopause even without a hot flash?
The early morning wake-up is driven by the convergence of declining progesterone, which normally calms the brain’s sleep receptors, and the body’s natural cortisol rise in the predawn hours. You do not need a hot flash to experience this disruption. It is a neurobiological event, and in The Busy Brain Cure I explain exactly why it happens and what you can do about it.
What labs should I ask my doctor for if I am having perimenopause sleep problems?
Ask for a full thyroid panel (not just TSH), a morning cortisol level, and a complete hormone panel that includes estradiol, progesterone, and testosterone. These labs give your doctor the full picture of what is driving your symptoms. Chapter 16 of The Busy Brain Cure includes a ready-to-use list you can bring to your appointment.
Is hormone replacement therapy safe for sleep problems in perimenopause?
For women who are candidates, HRT is one of the most evidence-based tools available for restoring sleep and protecting brain health during the menopausal transition. The risk landscape around HRT has been significantly reinterpreted since earlier studies. This is a conversation worth having directly with your physician based on your individual health history.
Are anxiety and temperature-related wake-ups the same thing in perimenopause?
From a neurological standpoint, yes. Both originate in the hypothalamus, where estrogen and progesterone loss creates hyperactivity in neurons that govern both thermal regulation and the sleep-wake cycle. They often feel like separate symptoms but share the same underlying driver.
What is CBT-I and why does it matter for menopausal sleep?
Cognitive Behavioral Therapy for Insomnia, or CBT-I, is a structured approach that retrains the thought patterns and behavioral habits driving chronic sleep disruption. In head-to-head clinical research, it outperformed estradiol, antidepressants, yoga, and omega-3 supplementation for improving sleep in menopausal women. Chapter 11 of The Busy Brain Cure breaks down the CBT-I steps as a practical sleep challenge you can start on your own.
When should disrupted sleep in my 40s prompt a doctor visit?
If you are consistently waking in the early morning hours, feeling unrefreshed regardless of sleep duration, or experiencing brain fog, mood changes, or memory difficulties, it is time for a thorough evaluation. Sleep apnea is frequently missed in women at midlife because the symptoms present differently than in men, so ask specifically whether you should be screened.